女性におけるファブリー病
ヘテロ接合体の女性は保因者にとどまるわけではありません。
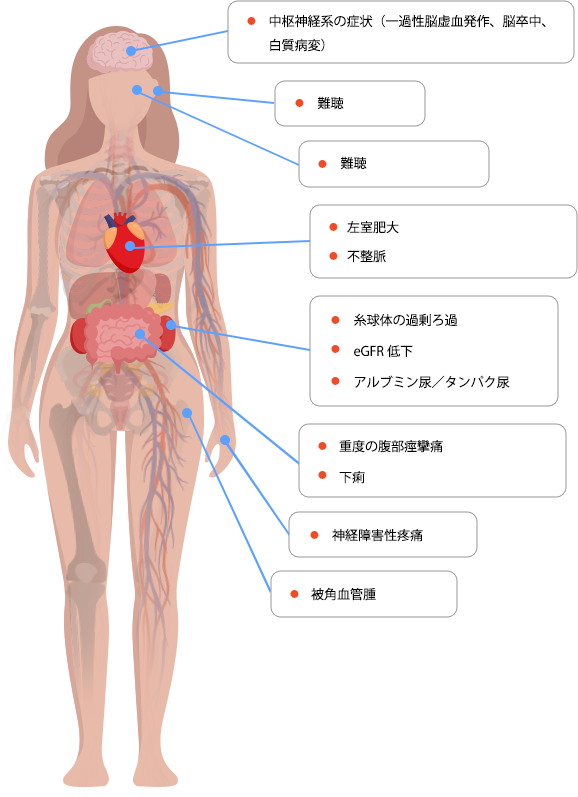
女性はGLA遺伝子変異の保因者であるにすぎない、というのはよくある誤解です。ヘテロ接合体の女性ではファブリー病の症状のあらわれ方が多様であり、無症状または軽症の場合もあれば、男性と同様に、心臓、腎臓、脳血管系の合併症をきたすなど全身の臓器に及ぶ重度の症状を呈する場合もあります1-3。
女性は最初に症状が出現してから診断されるまでに約11年かかります4。また、発症年齢が男性よりも遅い傾向があり5,6、通常、男性と比べてより長期にわたり、疾患を患うと報告されています7。